In this issue
- Arthritis Consumer Experts Survey Report on Arthritis and Exercise
- Survey goals
- Who were the Survey respondents?
- Exercise routine prior to an arthritis diagnosis
- Exercise routine after an arthritis diagnosis
- Exercise preferences
- What can health care providers do to support an exercise journey?
- Discussion
- Resources for your exercise journey
JointHealth™ insight Published May 2022


 People living with arthritis want or try to be involved in physical activities.
Some may focus on simple tasks in their daily life like working, doing chores around the house, doing yard work, and grocery shopping. While others may want to exercise regularly through brisk walking, participating in a ceremonial dance, tai chi, or yoga.
Many participate in more challenging forms of exercise, like road cycling and competitive team sports like basketball or beach volleyball. Many people with arthritis, however, also share common concerns: How much exercise is enough? How much is too much? What types of exercise are best, or should be avoided? Who can help create a personalized exercise plan?
People living with arthritis want or try to be involved in physical activities.
Some may focus on simple tasks in their daily life like working, doing chores around the house, doing yard work, and grocery shopping. While others may want to exercise regularly through brisk walking, participating in a ceremonial dance, tai chi, or yoga.
Many participate in more challenging forms of exercise, like road cycling and competitive team sports like basketball or beach volleyball. Many people with arthritis, however, also share common concerns: How much exercise is enough? How much is too much? What types of exercise are best, or should be avoided? Who can help create a personalized exercise plan?
 Making exercise and physical activity a priority
Making exercise and physical activity a priority
In 2018, the European Alliance of Associations for Rheumatology (EULAR) updated its recommendations for physical activity in people living with inflammatory arthritis and osteoarthritis. Physical activity is defined as any movement that is produced by the muscles that requires energy (i.e., any movement a person does). Physical activity includes exercise, sports, and physical activities done during daily living, such as gardening and active transportation. Exercise is planned, structured and repetitive activity with the goal to improve or maintain one’s physical fitness.
The EULAR guidelines for people aged 18-65 years living with arthritis are:
It is important that health care providers help their clients work exercise into their daily routine, understanding that they already spend time self-caring for their disease. Adding or increasing time spent for exercise can prove challenging for some.1
While the research literature tells us a lot about exercise, it is important to hear directly from people with arthritis. Arthritis Consumer Experts (ACE) conducted a Survey, from March 16, 2022 to April 5, 2022, to learn more about peoples’ exercise routines and preferences before and after their arthritis diagnosis and identify any barriers they have experienced when seeking exercise guidance and support from health care providers.
Survey goals
ACE members and subscribers have shared with us the many challenges to finding detailed information, and help, to guide safe exercise. With this survey, ACE’s goal was to identify gaps in exercise education, programming, and monitoring and how the healthcare system, health care providers, and patient organizations can better support an arthritis patient’s exercise journey.
How the Survey was conducted
Arthritis Consumer Experts conducted an online 30-question Survey of people living with a physician diagnosed form of arthritis between March 16, 2022 and April 5, 2022 in English and French. The Survey included questions on respondents’ exercise experience prior to and after their arthritis diagnosis. Throughout the Survey, respondents were able to provide additional comments about what would help improve their exercise journey. Data were analysed in aggregate by a data specialist.
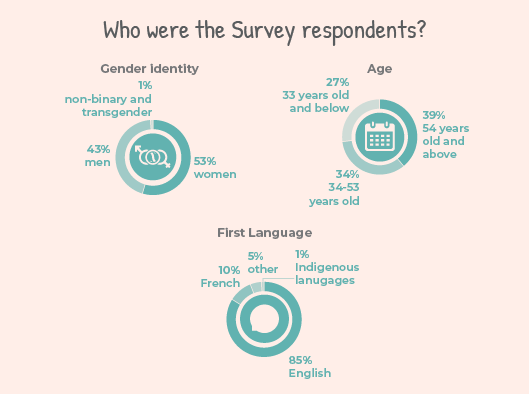 Who were the Survey respondents?
Who were the Survey respondents?
Arthritis Consumer Experts received 288 responses, including 270 in English and 18 in French (15 were Quebec residents).
Respondents were people who self-reported living with various forms of arthritis, including:
Nine in 10 respondents identified as women. This comes as no surprise as women are affected in greater proportions than men by most types of arthritis.
One in 10 respondents identified as black, Indigenous, or a person of colour. Nine in 10 respondents were white. This represents a significant gap in ethnic and racial representation. Representation refers to research studies where the research participants do not reflect the racial identity, ethnicity, age, or sex and gender of the population that's affected.
ACE is committed to continuing its work to bring equity to representation and knowledge translation and exchange for everyone in our community. To learn more about this topic, read this ACE article on who is and who is not represented in research.
Where respondents live
Thirty-four percent of Survey respondents reported living in British Columbia, followed by Ontario (29%), and Quebec (9%). There were respondents from all Canadian provinces and territories except for Yukon and Nunavut.
Respondents lived in both rural or small to medium sized, and urban communities:
Exercise routine prior to an arthritis diagnosis
To understand the bigger picture of respondents’ exercise experience, we asked Survey respondents about their exercise routine prior to their arthritis diagnosis. The four questions in this section revealed what types of exercise(s) respondents participated in, how frequently respondents exercised, how long they exercised for, and how challenging most of the exercise sessions were. What type of exercise did respondents
What type of exercise did respondents
participate in?
Survey respondents were asked what type of exercise they participated in and had the option to select all that apply. The top three types of exercises were recreational activities (70% of respondents), exercise programs or classes such as Pilates, yoga, dance or swimming lessons (45% of respondents), and individual exercise such as skiing or tennis (31% of respondents). These findings were similar for respondents no matter their type of arthritis, gender, race or ethnicity or where they lived. Nine per cent of respondents said they did not participate in any exercise prior to their arthritis diagnosis.
Other types of exercise that respondents selected were:
What respondents told us
When asked what type(s) of exercise they participated in prior to their arthritis diagnosis, here are some sample responses:
 Frequency, duration and intensity of exercise
Frequency, duration and intensity of exercise
Most respondents exercised 3 to 4 days per week (4 in 10 respondents), followed by 5 to 6 days per week (3 in 10 respondents) and 1 to 2 days per week (1 in 10 respondents). One in 10 respondents reported exercising daily, bi-weekly or rarely.
On average, the duration of each exercise session for Survey respondents were:
Exercise routine after an arthritis diagnosis Having the exercise discussion with health care providers
Having the exercise discussion with health care providers
When asked if a health care provider (HCP) discussed exercise at the time of or shortly after their arthritis diagnosis, 3 in 10 respondents said they had an exercise discussion with their HCP, but only general information was provided; 1 in 10 respondents said they had an exercise discussion with their HCP and their HCP suggested specific exercise and community resources for them. Five in 100 respondents living in rural communities said that they had the exercise discussion at the time or shortly after their arthritis diagnosis and, together with their HCP, have developed a new exercise routine.
One in 10 respondents said their HCP discussed exercise with them after they asked for information about it. Respondents living in rural communities were two-third less likely to say their HCP had the exercise discussion with them after they asked about it.
Two in 10 respondents reported that:
What respondents told us
Here are some selected comments from respondents about which health care provider talked to them about exercise and their type of arthritis:
 Changes to your exercise routine
Changes to your exercise routine
The Survey asked how respondents’ exercise routine changed after their diagnosis and they had the option to select all that apply. Nearly 9 out of 10 respondents said that their exercise routine changed after their arthritis diagnosis, compared to 1 out of 10 who said that their exercise routine remained the same (respondents in rural communities were two times more likely to say their exercise routine remained the same). Below are some Survey findings from this question:
When asked why their exercise routine changed after their arthritis diagnosis, here are a few respondents’ comments:
Exercise preferences
Three out of 10 respondents liked to exercise on their own, while 3 out of 100 selected “other” and explained:
Survey findings that indicate different significant responses among BIPOC respondents could be related to social determinants of health and the lack of culturally sensitive or appropriate approaches to supporting exercise or physical activity.
Research shows, for example, that Indigenous Peoples may experience challenges in participating in physical activity or exercise programs. Prominent barriers included a lack of transport, financial constraints, lack of time, and competing work, family or cultural commitments.2
Among respondents living in rural communities, they were only half as likely to be concerned they are doing the exercise incorrectly when compared to non-rural respondents. However, rural respondents were also two times more likely to be concerned that exercise will worsen their pain or report that they do not enjoy doing exercise.
What respondents told us
Many respondents shared personal comments about the challenges in their exercise journey:
 Finding exercise information and support
Finding exercise information and support
Forty-one per cent of respondents would like to get exercise information from digital resources on computer, phone or tablet; while 32% would like to get in-person advice or counselling, 17% would like to get written materials, and 10% selected “other”. Responses in the “other” section include:
Here are sample comments from respondents on what would be helpful to support them in starting or continuing their exercise journey:
 What can health care providers do to support an exercise journey?
What can health care providers do to support an exercise journey?
Five out of 10 respondents said they would like their health care provider to be involved in counselling on the importance and benefits of exercise. Eight out of 10 would like an HCP to design and create an exercise program with them, while 6 out of 10 would like an HCP to encourage them to exercise and 8 out of 10 wanted their HCP to support them to stay motivated.
Six out of 10 respondents found it helpful to have an HCP check in with them about their exercise journey; while 2 out of 10 are unsure and 2 out of 10 do not find it helpful to have an HCP check in with them about their exercise journey.
BIPOC respondents were one and a half more times likely to say “encouraging me to exercise” would help them in their exercise journey.
Out of the respondents who said they found it helpful or are unsure if they found it helpful, 3 out of 10 would like their HCP to check in with them quarterly, 3 out of 10 would like monthly check ins, 2 out of 10 would like weekly check ins, 1 out of 10 would like bi-annual check ins, and 1 out of 10 would like annual check ins. The top preference in the BIPOC community was that they preferred to have weekly check ins, compared to non-BIPOC community respondents who preferred to have quarterly check ins.
When asked what member of your health care team should be responsible for offering advice and building a personalized exercise routine with you, Survey respondents selected all that applied to them from a list. Respondents’ top five answer choices were:
What respondents told us
Here are some comments from respondents to the question what members of their health care team should be responsible for offering advice and building a personalized exercise routine:
 Discussion
Discussion
What we learned
Let’s face it, exercising consistently is difficult. Making time and taking the first steps are challenging enough but staying active during the waves of arthritis pain and fatigue takes extraordinary commitment and support.
ACE strongly believes that individuals living with arthritis should not have to do it alone. For people living with arthritis, exercise is an evidence-based medicine that helps to control and reduce symptoms such as pain, fatigue and anxiety. Combined, this all translates to a more meaningful and productive life. A large majority of ACE’s Survey respondents report engaging in recreational activities, exercise programs or classes, and individual activities prior to their arthritis diagnosis. The main reasons for exercise routines to change after receiving an arthritis diagnosis were pain, fatigue, lack of confidence and motivation. These findings suggest that many respondents understand the benefits of exercise, yet they experience significant barriers that are not being addressed by the health care system.
Finding support for starting or staying on an exercise program is critical. The Johns Hopkins Arthritis Center’s PACE (Physician-Based Assessment and Counseling for Exercise) Project found that 3-5 minute of doctor-patient counseling sessions about exercise increased physical activity among patients. This study also found that 80% of physicians reported that their patients were “receptive” or “very receptive” to physical activity, and more than 50% of providers perceived that their patients did increase their level of physical activity after this brief discussion.3
While exercise is an individual’s responsibility, supporting exercise is the role of all members of a patient’s health care team. In terms of programs and resources, Survey respondents want to join arthritis exercise class(es) in the community, have access to an exercise coach, as well as detailed video instructions on how to do each exercise. Survey findings also reflect the unique needs of diverse respondents. For example, BIPOC respondents are twice as likely to be concerned about doing exercise incorrectly and want additional support from an exercise coach. Overall, respondents want to have their health care providers engaged and invested in their physical activity. More than half of respondents would like to have an HCP check in with them about exercise on a quarterly or monthly basis. Unfortunately, only a handful of respondents living in rural communities have spoken to their HCP about exercise, which highlights a gap due to where the respondents live. What you can do
What you can do
In terms of exercise, remember that some is better than none. Over time, taking the stairs or going for a brisk walk around the block adds up. If you are engaged in sports or activities that you do not want to give up, bring it up and speak honestly with your HCPs about your desires and needs. Keep in mind that you may have to compromise or modify how you do certain activities, but you do not necessarily have to give them up. If you are completely new to exercise or getting back into it, then start small and work on consistency before you move on. For instance, do ten push ups at your counter while waiting for your kettle to boil and do it every day until it becomes a habit. Lastly, ask yourself what knowledge and skills do I need to learn? Where do I go to gain access to programs and resources? And who can support me on my journey? Use this information to build a sustainable exercise plan. As with weather, plan for the worst but hope for the best.
Resources for your exercise journey
To help you on your exercise journey, the following resources may be helpful:
References
Listening to you
We hope you find this information of use. Please tell us what you think by writing to us or emailing us at feedback@jointhealth.org. Through your ongoing and active participation, ACE can make its work more relevant to all Canadians living with arthritis.
Update your email or postal address
Please let us know of any changes by contacting ACE at feedback@jointhealth.org. This will ensure that you continue to receive your free email or print copy of JointHealth™ insight.
Arthritis Consumer Experts (ACE)
Who We Are
Arthritis Consumer Experts (ACE) and its team members acknowledge that they gather and work on the traditional, ancestral and unceded territory of the Coast Salish peoples -ʷməθkʷəy̓əm (Musqueam), Sḵwx̱wú7mesh (Squamish), and Səl̓ílwətaʔ/Selilwitulh (Tsleil-Waututh) Nations.
Arthritis Consumer Experts (ACE) operates as a non-profit and provides free research based education and information to Canadians with arthritis. We help (em)power people living with all forms of arthritis to take control of their disease and to take action in healthcare and research decision making. ACE activities are guided by its members and led by people with arthritis, scientific and medical experts on the ACE Advisory Board. To learn more about ACE, visit www.jointhealth.org
Disclosures
Over the past 12 months, ACE received grants-in-aid from: Amgen Canada, Arthritis Research Canada, Canadian Biosimilars Forum, Canadian Rheumatology Association, Eli Lilly Canada, Fresenius Kabi Canada, Merck Canada, Novartis Canada, Organon Canada, Pfizer Canada, Sandoz Canada, Teva Canada, UCB Canada and the University of British Columbia.
ACE also received unsolicited donations from its community members (people with arthritis) across Canada.
ACE thanks funders for their support to help the nearly 6 million Canadians living with osteoarthritis, rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis and the many other forms of the disease.
Disclaimer
The material contained on this website is provided for general information only. This website should not be relied on to suggest a course of treatment for a particular individual or as a substitute for consultation with qualified health professionals who are familiar with your individual medical needs. Should you have any healthcare related questions, you should contact your physician. You should never disregard medical advice or delay in seeking it because of something you have read on this or any website.
This site may provide links to other Internet sites only for the convenience of World Wide Web users. ACE is not responsible for the availability or content of these external sites, nor does ACE endorse, warrant or guarantee the products, services or information described or offered at these other Internet sites.
Although the information presented on this website is believed to be accurate at the time it is posted, this website could include inaccuracies, typographical errors or out-of-date information. This website may be changed at any time without prior notice.
People living with arthritis want or try to be involved in physical activities.
Some may focus on simple tasks in their daily life like working, doing chores around the house, doing yard work, and grocery shopping. While others may want to exercise regularly through brisk walking, participating in a ceremonial dance, tai chi, or yoga.
Many participate in more challenging forms of exercise, like road cycling and competitive team sports like basketball or beach volleyball. Many people with arthritis, however, also share common concerns: How much exercise is enough? How much is too much? What types of exercise are best, or should be avoided? Who can help create a personalized exercise plan?
Making exercise and physical activity a priorityIn 2018, the European Alliance of Associations for Rheumatology (EULAR) updated its recommendations for physical activity in people living with inflammatory arthritis and osteoarthritis. Physical activity is defined as any movement that is produced by the muscles that requires energy (i.e., any movement a person does). Physical activity includes exercise, sports, and physical activities done during daily living, such as gardening and active transportation. Exercise is planned, structured and repetitive activity with the goal to improve or maintain one’s physical fitness.
The EULAR guidelines for people aged 18-65 years living with arthritis are:
- Do moderate intensity aerobic physical activity for 30 minutes or 5 days per week; or,
- Do vigorous intensity aerobic activity for 20 minutes or 3 days per week.
It is important that health care providers help their clients work exercise into their daily routine, understanding that they already spend time self-caring for their disease. Adding or increasing time spent for exercise can prove challenging for some.1
While the research literature tells us a lot about exercise, it is important to hear directly from people with arthritis. Arthritis Consumer Experts (ACE) conducted a Survey, from March 16, 2022 to April 5, 2022, to learn more about peoples’ exercise routines and preferences before and after their arthritis diagnosis and identify any barriers they have experienced when seeking exercise guidance and support from health care providers.
Survey goals
ACE members and subscribers have shared with us the many challenges to finding detailed information, and help, to guide safe exercise. With this survey, ACE’s goal was to identify gaps in exercise education, programming, and monitoring and how the healthcare system, health care providers, and patient organizations can better support an arthritis patient’s exercise journey.
How the Survey was conducted
Arthritis Consumer Experts conducted an online 30-question Survey of people living with a physician diagnosed form of arthritis between March 16, 2022 and April 5, 2022 in English and French. The Survey included questions on respondents’ exercise experience prior to and after their arthritis diagnosis. Throughout the Survey, respondents were able to provide additional comments about what would help improve their exercise journey. Data were analysed in aggregate by a data specialist.
| ACE extends its sincere thanks to the people who took time to participate in this important community-led research and to our community partners who helped promote the Survey. |
Who were the Survey respondents?Arthritis Consumer Experts received 288 responses, including 270 in English and 18 in French (15 were Quebec residents).
Respondents were people who self-reported living with various forms of arthritis, including:
- rheumatoid arthritis (39%)
- osteoarthritis (35%)
- ankylosing spondylitis (9%)
- other (5%)
- psoriatic arthritis (4%)
- do not know what type of arthritis they have (3%)
- Sjögren’s syndrome (2%)
- gout (1%)
- lupus (1%)
- juvenile idiopathic arthritis (1%)
- polymyalgia rheumatica (1%)
- fibromyalgia (less than 1%)
- adult-onset Still’s disease (less than 1%)
- scleroderma (less than 1%)
Nine in 10 respondents identified as women. This comes as no surprise as women are affected in greater proportions than men by most types of arthritis.
One in 10 respondents identified as black, Indigenous, or a person of colour. Nine in 10 respondents were white. This represents a significant gap in ethnic and racial representation. Representation refers to research studies where the research participants do not reflect the racial identity, ethnicity, age, or sex and gender of the population that's affected.
ACE is committed to continuing its work to bring equity to representation and knowledge translation and exchange for everyone in our community. To learn more about this topic, read this ACE article on who is and who is not represented in research.
|
Are you a member of the black, Indigenous, and people of colour community and interested in addressing health inequities? Please email us at feedback@jointhealth.org for collaboration opportunities. |
Thirty-four percent of Survey respondents reported living in British Columbia, followed by Ontario (29%), and Quebec (9%). There were respondents from all Canadian provinces and territories except for Yukon and Nunavut.
Respondents lived in both rural or small to medium sized, and urban communities:
- 55% of respondents live in large urban centres with population of 100,000 or more
- 45% of respondents live in either rural (population of 15,999 or less) or small to medium sized population centres (population of 16,000 to 99,999)
- 11-25km (26%)
- 26-50km (12%)
- 51-100km (7%)
- 101-250km (7%)
- 251-500km (3%)
- 500km or more (1%)
Exercise routine prior to an arthritis diagnosis
To understand the bigger picture of respondents’ exercise experience, we asked Survey respondents about their exercise routine prior to their arthritis diagnosis. The four questions in this section revealed what types of exercise(s) respondents participated in, how frequently respondents exercised, how long they exercised for, and how challenging most of the exercise sessions were.
What type of exercise did respondents participate in?
Survey respondents were asked what type of exercise they participated in and had the option to select all that apply. The top three types of exercises were recreational activities (70% of respondents), exercise programs or classes such as Pilates, yoga, dance or swimming lessons (45% of respondents), and individual exercise such as skiing or tennis (31% of respondents). These findings were similar for respondents no matter their type of arthritis, gender, race or ethnicity or where they lived. Nine per cent of respondents said they did not participate in any exercise prior to their arthritis diagnosis.
Other types of exercise that respondents selected were:
- Cardiovascular training such as running, jogging, or road and stationary cycling (30%)
- Strength based training such as weightlifting (29%)
- Other such as walking, playing with children, gardening or tai-chi (18%)
- Team sports such as curling, soccer, basketball or volleyball (9%)
What respondents told us
When asked what type(s) of exercise they participated in prior to their arthritis diagnosis, here are some sample responses:
|
“I did a variety of moderate forms, but no regular pattern prior to diagnosis due to painful conditions so it depended how I felt that day. Cycling or walking mostly, occasionally some form of sports like badminton or volleyball. Skiing a few times and horseback riding but painful days prevented much more than that.” – Person living with ankylosing spondylitis “I do the stretching exercises my chiropractor has suggested. I’ve added balancing exercise, and chi gong.” – Person living with spinal stenosis, arthritis, and osteoporosis “Virtual exercise classes for people with diabetes and also strength training exercises and I walk every day.” – Person living with osteoarthritis |
Frequency, duration and intensity of exerciseMost respondents exercised 3 to 4 days per week (4 in 10 respondents), followed by 5 to 6 days per week (3 in 10 respondents) and 1 to 2 days per week (1 in 10 respondents). One in 10 respondents reported exercising daily, bi-weekly or rarely.
On average, the duration of each exercise session for Survey respondents were:
- 46-60 minutes long (33%)
- 31-45 minutes long (24%)
- 16-30 minutes long (23%)
- 0-15 minutes long (10%)
- More than 60 minutes long (10%)
- Half of the respondents found their exercise session to be “light” intensity – they can have a conversation while doing this activity
- Close to half (47%) found their exercise session to be “moderate” intensity – they find it difficult to have a conversation while doing this activity
- 3% found their exercise session to be “high” intensity – they find it impossible to have a conversation while doing this activity
Exercise routine after an arthritis diagnosis
Having the exercise discussion with health care providersWhen asked if a health care provider (HCP) discussed exercise at the time of or shortly after their arthritis diagnosis, 3 in 10 respondents said they had an exercise discussion with their HCP, but only general information was provided; 1 in 10 respondents said they had an exercise discussion with their HCP and their HCP suggested specific exercise and community resources for them. Five in 100 respondents living in rural communities said that they had the exercise discussion at the time or shortly after their arthritis diagnosis and, together with their HCP, have developed a new exercise routine.
One in 10 respondents said their HCP discussed exercise with them after they asked for information about it. Respondents living in rural communities were two-third less likely to say their HCP had the exercise discussion with them after they asked about it.
Two in 10 respondents reported that:
- there was no discussion at all about exercise
- did not have the exercise conversation with their HCP but feel confident in their own knowledge, skills and experience to continue participating in exercise
- Rheumatologist (37%)
- Physiotherapist (37%)
- Family doctor or physician (35%)
- Other (16%)
- Fitness professional (9%)
- Occupational therapist (9%)
- Chiropractor (9%)
- Rheumatology nurse (4%)
- Kinesiologist (4%)
- I do not have access to a health care provider (3%)
- Dietitian (2%)
- Psychologist (1%)
- Pharmacist (less than 1%)
What respondents told us
Here are some selected comments from respondents about which health care provider talked to them about exercise and their type of arthritis:
|
“The discussion was about 15 years after diagnosis.” – Person living with rheumatoid arthritis “After my diagnosis, a physiotherapist gave me some stretches to do and mostly put me on a heat pad for my appt.” – Person living with ankylosing spondylitis “Was referred to the local Arthritis Centre who then suggested seeing one of their physiotherapists.” – Person living with rheumatoid arthritis |
Changes to your exercise routineThe Survey asked how respondents’ exercise routine changed after their diagnosis and they had the option to select all that apply. Nearly 9 out of 10 respondents said that their exercise routine changed after their arthritis diagnosis, compared to 1 out of 10 who said that their exercise routine remained the same (respondents in rural communities were two times more likely to say their exercise routine remained the same). Below are some Survey findings from this question:
- Exercising at a less challenging level compared to at a more challenging level (33% vs 7%)
- Exercising less frequently compared to more frequently (25% vs 18%)
- Doing less of a variety of exercises compared to doing more of a variety of exercises (15% vs 14%)
- I stopped or reduced my exercise on my own due to disease activity and symptoms such as fatigue and pain (56%)
- I was advised by an HCP to begin or increase exercise (14%)
- I stopped because it was difficult to keep myself engaged and motivated (14%)
When asked why their exercise routine changed after their arthritis diagnosis, here are a few respondents’ comments:
|
“I was concerned my health would declined more rapidly if I didn't start exercising more intentionally so I started exercising.” – Person living with juvenile idiopathic arthritis “Some days I can't do as much as I did before too tired, or too much pain. Symptoms have worsened.” – Person living with psoriatic arthritis “I increased exercise because I felt it improved my arthritis. I added routines, especially stretching, physio exercises, weight lifting exercises, to strengthen muscle to support the joints. I eventually learned that movement feeds the joints and helps the joints eliminate wastes.” – Person living with ankylosing spondylitis “I participated in a study at the University of Calgary about the benefits of cardiovascular exercise for patients with arthritis.” – Person living with rheumatoid arthritis “Exercise venues not available to me due to pandemic and restrictions due to immuno- compromised status.” – Person living with rheumatoid arthritis |
Three out of 10 respondents liked to exercise on their own, while 3 out of 100 selected “other” and explained:
- “On my own, but in a gym so I can use the equipment. Not interested in classes.”
- “I like to be accompanied by a dedicated trainer/physio.”
- “Due to the pandemic, I have been exercising on my own at home with a weekly zoom check in with my kinesiologist.”
- Pain during or after exercise (53%)
- Feeling tired or fatigued (26%)
- Concerns about doing exercise incorrectly (23%)
- Lack of motivation to exercise (19%)
- Concerned exercise worsened pain (18%)
Survey findings that indicate different significant responses among BIPOC respondents could be related to social determinants of health and the lack of culturally sensitive or appropriate approaches to supporting exercise or physical activity.
Research shows, for example, that Indigenous Peoples may experience challenges in participating in physical activity or exercise programs. Prominent barriers included a lack of transport, financial constraints, lack of time, and competing work, family or cultural commitments.2
Among respondents living in rural communities, they were only half as likely to be concerned they are doing the exercise incorrectly when compared to non-rural respondents. However, rural respondents were also two times more likely to be concerned that exercise will worsen their pain or report that they do not enjoy doing exercise.
What respondents told us
Many respondents shared personal comments about the challenges in their exercise journey:
|
“I do not notice an improvement and no one is monitoring my progress so maintaining motivation is challenging.” – Person living with juvenile idiopathic arthritis “I've had to modify some exercises like yoga poses due to joint weakness or deformity, but I still enjoy exercise and always feel better afterwards.” – Person living with rheumatoid arthritis “Fatigue can make it difficult to start exercise, even though I know from past experience that I receive benefit from exercise. Over use injury in the past has seemed to contribute to arthritis flares, so finding the right level of intensity and quantity is important.” – Person living with ankylosing spondylitis “Exercise that was supposed to help my osteoarthritis created other problems and pain in other parts of the body. I could not find a therapist that would help me holistically and create an exercise program that will fit my abilities and restrictions. Every provider I tried working with pushed me to the point of extreme pain. They all said it's just arthritis and I should not complain about pain levels.” – Person living with osteoarthritis |
Finding exercise information and supportForty-one per cent of respondents would like to get exercise information from digital resources on computer, phone or tablet; while 32% would like to get in-person advice or counselling, 17% would like to get written materials, and 10% selected “other”. Responses in the “other” section include:
- all of the above
- from an in-person physio visit
- clear hard copy instructions from physio or OT or kinesiologist
- access to a coach person for consultation and advice and review
- Joining an arthritis exercise program/class in my community (44%)
- Having an exercise coach (38%)
- Detailed video instructions on how to do each exercise (31%)
- Detailed handouts with pictures on how to do each exercise (27%)
- Having affordable access to exercise equipment and facilities (27%)
- Having a detailed consultation with my health care providers (25%)
- Joining a support group to keep me motivated (22%)
- Having a reward system (12%)
- BIPOC respondents were twice as likely to say having an exercise coach will help support their exercise journey
- BIPOC respondents were 3 times more likely to say having a reward system will help support their exercise journey
Here are sample comments from respondents on what would be helpful to support them in starting or continuing their exercise journey:
|
“Virtual online group or individual classes at various times of the day that I could do from home.” – Person living with ankylosing spondylitis “Having input when my exercise requirements need to be changed. This has been an on-going problem with the chronic conditions I have, not just arthritis.” – Person living with Sjögren's syndrome “Specific goals always motivate me. ie: right now I am addressing lots of exercises to improve functions such as squatting to make being around my grandchildren more fun and to enable me to go camping (on the ground) easier.” – Person living with rheumatoid arthritis “I've tried working with personal trainers but few understand rheumatoid had success with own who was amazing but otherwise got into situations where they were recommending things that exacerbated RA. Group classes are out as group instructors rarely able to accommodate RA limitations.” – Person living with rheumatoid arthritis |
What can health care providers do to support an exercise journey?Five out of 10 respondents said they would like their health care provider to be involved in counselling on the importance and benefits of exercise. Eight out of 10 would like an HCP to design and create an exercise program with them, while 6 out of 10 would like an HCP to encourage them to exercise and 8 out of 10 wanted their HCP to support them to stay motivated.
Six out of 10 respondents found it helpful to have an HCP check in with them about their exercise journey; while 2 out of 10 are unsure and 2 out of 10 do not find it helpful to have an HCP check in with them about their exercise journey.
BIPOC respondents were one and a half more times likely to say “encouraging me to exercise” would help them in their exercise journey.
Out of the respondents who said they found it helpful or are unsure if they found it helpful, 3 out of 10 would like their HCP to check in with them quarterly, 3 out of 10 would like monthly check ins, 2 out of 10 would like weekly check ins, 1 out of 10 would like bi-annual check ins, and 1 out of 10 would like annual check ins. The top preference in the BIPOC community was that they preferred to have weekly check ins, compared to non-BIPOC community respondents who preferred to have quarterly check ins.
When asked what member of your health care team should be responsible for offering advice and building a personalized exercise routine with you, Survey respondents selected all that applied to them from a list. Respondents’ top five answer choices were:
- Physiotherapist (66%)
- Family doctor or physician (42%)
- Fitness professional, such as a personal trainer, yoga instructor or group fitness coach (37%)
- Rheumatologist (37%)
- Occupational therapist (23%)
What respondents told us
Here are some comments from respondents to the question what members of their health care team should be responsible for offering advice and building a personalized exercise routine:
|
“Don't have a health care team. Family doctor is kind of useless and only good for refills of my prescriptions.” – Person living with osteoarthritis “Access to a professional not covered (ie. kinesiologist or fitness professional) is for the most part impossible due to my remote location and low income.” – Person living with ankylosing spondylitis “Perhaps just having the right questions to ask when I see any of my health care team - I don't think the onus should be with just one specific person and I also think I need to take some responsibility for my wellness.” – Person living with rheumatoid arthritis “Living in a rural area with a different/ older family doctor now versus earlier - I no long have access to a rheumatologist, o.t. or p.t. or even community activities/ community members due to covid and lack now of community transportation as it has been discontinued.” – Person living with osteoa |
DiscussionWhat we learned
Let’s face it, exercising consistently is difficult. Making time and taking the first steps are challenging enough but staying active during the waves of arthritis pain and fatigue takes extraordinary commitment and support.
ACE strongly believes that individuals living with arthritis should not have to do it alone. For people living with arthritis, exercise is an evidence-based medicine that helps to control and reduce symptoms such as pain, fatigue and anxiety. Combined, this all translates to a more meaningful and productive life. A large majority of ACE’s Survey respondents report engaging in recreational activities, exercise programs or classes, and individual activities prior to their arthritis diagnosis. The main reasons for exercise routines to change after receiving an arthritis diagnosis were pain, fatigue, lack of confidence and motivation. These findings suggest that many respondents understand the benefits of exercise, yet they experience significant barriers that are not being addressed by the health care system.
Finding support for starting or staying on an exercise program is critical. The Johns Hopkins Arthritis Center’s PACE (Physician-Based Assessment and Counseling for Exercise) Project found that 3-5 minute of doctor-patient counseling sessions about exercise increased physical activity among patients. This study also found that 80% of physicians reported that their patients were “receptive” or “very receptive” to physical activity, and more than 50% of providers perceived that their patients did increase their level of physical activity after this brief discussion.3
While exercise is an individual’s responsibility, supporting exercise is the role of all members of a patient’s health care team. In terms of programs and resources, Survey respondents want to join arthritis exercise class(es) in the community, have access to an exercise coach, as well as detailed video instructions on how to do each exercise. Survey findings also reflect the unique needs of diverse respondents. For example, BIPOC respondents are twice as likely to be concerned about doing exercise incorrectly and want additional support from an exercise coach. Overall, respondents want to have their health care providers engaged and invested in their physical activity. More than half of respondents would like to have an HCP check in with them about exercise on a quarterly or monthly basis. Unfortunately, only a handful of respondents living in rural communities have spoken to their HCP about exercise, which highlights a gap due to where the respondents live.
What you can doIn terms of exercise, remember that some is better than none. Over time, taking the stairs or going for a brisk walk around the block adds up. If you are engaged in sports or activities that you do not want to give up, bring it up and speak honestly with your HCPs about your desires and needs. Keep in mind that you may have to compromise or modify how you do certain activities, but you do not necessarily have to give them up. If you are completely new to exercise or getting back into it, then start small and work on consistency before you move on. For instance, do ten push ups at your counter while waiting for your kettle to boil and do it every day until it becomes a habit. Lastly, ask yourself what knowledge and skills do I need to learn? Where do I go to gain access to programs and resources? And who can support me on my journey? Use this information to build a sustainable exercise plan. As with weather, plan for the worst but hope for the best.
Resources for your exercise journey
To help you on your exercise journey, the following resources may be helpful:
- Arthritis At Home: Exercise Snacks with Dr. Jasmin Ma
- 3 Fab Facts for Happy Joints
- The GLA:D® program
- 30-Day Exercise Challenge for Arthritis
- 24-Hour Movement Guidelines
References
| 1 | 2018 EULAR recommendations for physical activity in people with inflammatory arthritis and osteoarthritis: https://bit.ly/38px0id |
| 2 | Bridget Allen, et al. Facilitators and Barriers to Physical Activity and Sport Participation Experienced by Aboriginal and Torres Strait Islander Adults: A Mixed Method Review |
| 3 | John Hopkins Arthritis Center: Role of Exercise in Arthritis Management: https://www.hopkinsarthritis.org/patient-corner/disease-management/role-of-exercise-in-arthritis-management/ |
Listening to you
We hope you find this information of use. Please tell us what you think by writing to us or emailing us at feedback@jointhealth.org. Through your ongoing and active participation, ACE can make its work more relevant to all Canadians living with arthritis.
Update your email or postal address
Please let us know of any changes by contacting ACE at feedback@jointhealth.org. This will ensure that you continue to receive your free email or print copy of JointHealth™ insight.
Arthritis Consumer Experts (ACE)
Who We Are
Arthritis Consumer Experts (ACE) and its team members acknowledge that they gather and work on the traditional, ancestral and unceded territory of the Coast Salish peoples -ʷməθkʷəy̓əm (Musqueam), Sḵwx̱wú7mesh (Squamish), and Səl̓ílwətaʔ/Selilwitulh (Tsleil-Waututh) Nations.
Arthritis Consumer Experts (ACE) operates as a non-profit and provides free research based education and information to Canadians with arthritis. We help (em)power people living with all forms of arthritis to take control of their disease and to take action in healthcare and research decision making. ACE activities are guided by its members and led by people with arthritis, scientific and medical experts on the ACE Advisory Board. To learn more about ACE, visit www.jointhealth.org
Disclosures
Over the past 12 months, ACE received grants-in-aid from: Amgen Canada, Arthritis Research Canada, Canadian Biosimilars Forum, Canadian Rheumatology Association, Eli Lilly Canada, Fresenius Kabi Canada, Merck Canada, Novartis Canada, Organon Canada, Pfizer Canada, Sandoz Canada, Teva Canada, UCB Canada and the University of British Columbia.
ACE also received unsolicited donations from its community members (people with arthritis) across Canada.
ACE thanks funders for their support to help the nearly 6 million Canadians living with osteoarthritis, rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis and the many other forms of the disease.
Disclaimer
The material contained on this website is provided for general information only. This website should not be relied on to suggest a course of treatment for a particular individual or as a substitute for consultation with qualified health professionals who are familiar with your individual medical needs. Should you have any healthcare related questions, you should contact your physician. You should never disregard medical advice or delay in seeking it because of something you have read on this or any website.
This site may provide links to other Internet sites only for the convenience of World Wide Web users. ACE is not responsible for the availability or content of these external sites, nor does ACE endorse, warrant or guarantee the products, services or information described or offered at these other Internet sites.
Although the information presented on this website is believed to be accurate at the time it is posted, this website could include inaccuracies, typographical errors or out-of-date information. This website may be changed at any time without prior notice.

